Causes
Chlamydia is caused by the obligate intracellular bacterium Chlamydia trachomatis.
Clinical presentation
Chlamydia is usually asymptomatic.
People with a penis
Symptoms - urethral discharge, dysuria and/or anorectal symptoms (Refer to Proctitis treatment guidelines).
Complications - epididymo-orchitis (for people with testes). Refer to Epididymo-orchitis treatment guidelines.
People with a vagina
- Symptoms - vaginal discharge, dysuria, post coital bleeding and/or anorectal symptoms (Refer to Proctitis treatment guidelines).
- Complications:
- Pelvic inflammatory disease (PID, in people with a cervix, uterus, fallopian tubes or ovaries) - chronic pelvic pain, ectopic pregnancy and infertility. Refer to PID treatment guidelines.
- Pregnant person to child transmission - neonatal conjunctivitis and pneumonitis.
Diagnosis
People with a penis
| Test | Site/Specimen | Comments |
|---|---|---|
| NAAT | FPU | If gay, bisexual or other men who have sex with men (GBMSM), also collect anal and pharyngeal swabs even if asymptomatic at these sites. |
| NAAT | Anorectal swab |
If GBMSM, and patient declines anal examination or has no anorectal symptoms, instruct in self-collection. Self-collection is as sensitive as swabs taken by a clinician and may be preferred by some people. |
| NAAT | Pharyngeal swab | Collect if GBMSM. Self-collection is as sensitive as swabs taken by a clinician and may be preferred by some people. |
People with a vagina
| Test | Site/Specimen | Comments |
|---|---|---|
| NAAT | Endocervical swab | Best test if examined. |
| NAAT | Self-collected vaginal swab |
As sensitive as clinician taken swabs, and are acceptable to many people. |
| NAAT | FPU | If endocervical swab/self-collected vaginal swab cannot be taken, for example after a hysterectomy, or in clients with a neovagina. Not as sensitive as self-collected vaginal swab. |
| NAAT | Anorectal swab |
If patient has had anal sex or has anorectal symptoms. If patient declines anal examination, refer patient for testing at a sexual health centre. |
If a chlamydia result is equivocal or inhibitors are present the test should be repeated. If the initial test was a urine sample, the repeat test should be performed by taking a urethral swab as the inhibitors may persist in the urine.
Management
Index patient
Chlamydia is notifiable to the Victorian Health Department by laboratories.
| Condition | First-line treatment | Alternative |
|---|---|---|
| Uncomplicated genital or pharyngeal infection |
Doxycycline 100mg per oral, twice daily for 7 days. |
Azithromycin 1g per oral, stat. Consider for patients likely to be nonadherent to doxycycline. |
| Anorectal infection |
Doxycycline 100mg per oral, twice daily for 7 days. If symptomatic, consider LGV Refer to LGV treatment guidelines Refer to Proctitis treatment guidelines |
Azithromycin 1g per oral, stat, and repeat in 12-24 hours. Doxycycline is superior to azithromycin for anorectal chlamydia. Perform a test of cure if using azithromycin in those with anorectal infection (see below). |
| Pelvic inflammatory disease |
Consider PID when chlamydia is diagnosed in a patient with female reproductive organs. |
|
| Epididymo-orchitis | Refer to Epididymo-orchitis treatment guidelines | |
| Pregnant women |
Azithromycin 1g PO, stat Doxycycline is contraindicated. |
If azithromycin is contraindicated: Amoxycillin 500mg PO, 3 times a day for 7 days OR Erythromycin ethylsuccinate (EES) 800mg PO, 4 times a day for 7 days OR Erythromycin ethylsuccinate (EES) 400mg PO, 4 times a day for 14 days |
Notification
Chlamydia is a notifiable disease in all Australian states/territories. The diagnosing clinician and/or the pathology laboratory is responsible for notification, depending on the jurisdiction. Pathology laboratories are responsible for notification in Victoria.
Partner management and patient delivered partner therapy
See link below:
Follow up
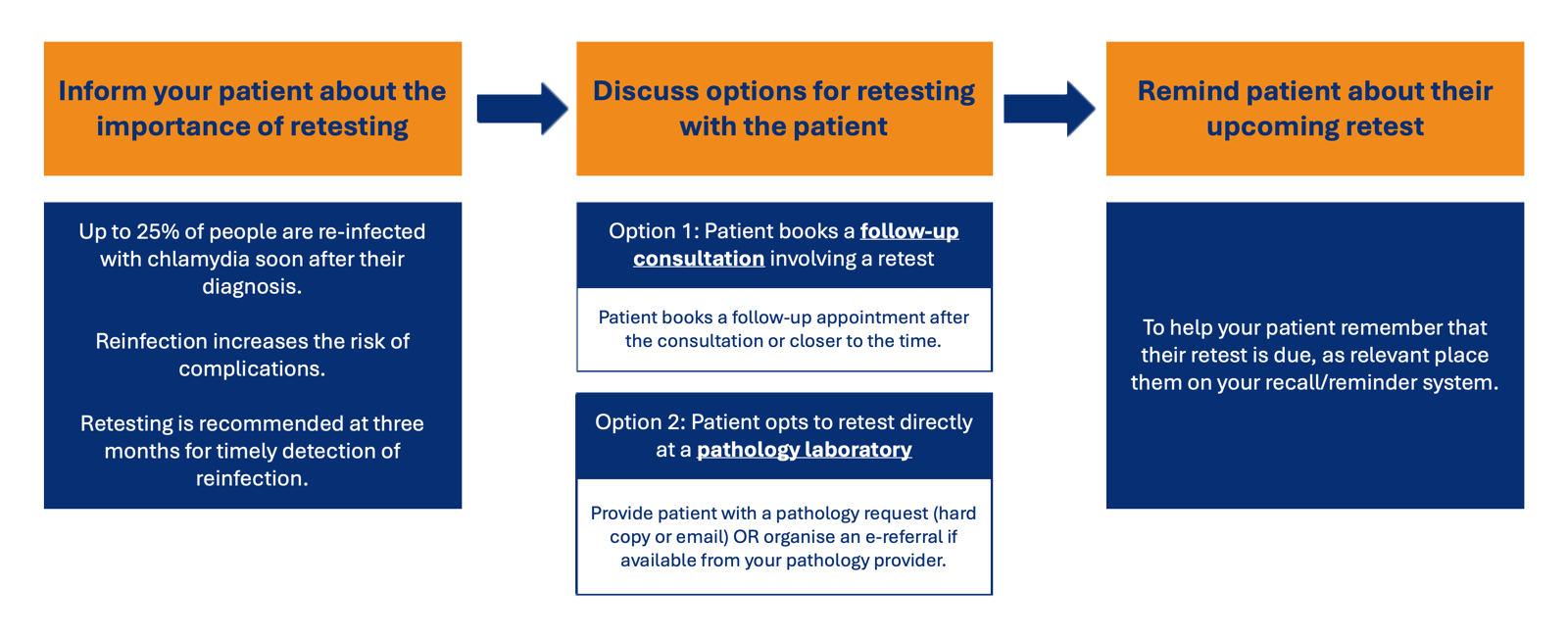
- A test for re-infection is recommended 3 months post-treatment to detect re-infection as re-infection is most common within three months of the initial infection.
- A test of cure is not routinely recommended except in:
- Pregnant people, and
- Anorectal infection treated with Azithromycin.
- If a test of cure is performed, it should not be done within 4 weeks post-treatment to prevent false positive due to persistent chlamydia DNA.
Disclaimer
We recognise that gender identity is fluid. In our treatment guidelines, the words and language we use to describe genitals and gender are based on the sex assigned at birth.
The content of these treatment guidelines is for information purposes only. The treatment guidelines are generic in character and should be applied to individuals only as deemed appropriate by the treating practitioner on a case by case basis. Alfred Health, through MSHC, does not accept liability to any person for the information or advice (or the use of such information or advice) which is provided through these treatment guidelines.
The information contained within these treatment guidelines is provided on the basis that all persons accessing the treatment guidelines undertake responsibility for assessing the relevance and accuracy of the content and its suitability for a particular patient. Responsible use of these guidelines requires that the prescriber is familiar with contraindications and precautions relevant to the various pharmaceutical agents recommended herein.